| Issue |
Int. J. Metrol. Qual. Eng.
Volume 8, 2017
|
|
|---|---|---|
| Article Number | 17 | |
| Number of page(s) | 15 | |
| DOI | https://doi.org/10.1051/ijmqe/2017015 | |
| Published online | 30 May 2017 | |
Review
X-ray computed tomography and additive manufacturing in medicine: a review
1
Manufacturing Metrology Team, Additive Manufacturing and 3D Printing Research Group, University of Nottingham,
Nottingham
NG7 2RD, UK
2
Bioengineering Research Group, University of Nottingham,
Nottingham
NG7 2RD, UK
⁎ Corresponding author: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
22
February
2017
Accepted:
2
May
2017
Abstract
The use of X-ray computed tomography (XCT) with additive manufacture (AM) within a medical context is examined in this review. The seven AM process families and various XCT scanning techniques are explained in brief, and the use of these technologies together is detailed over time. The transition of these technologies from a simple method of medical modelling to a robust method of customised implant manufacture is described, and the state-of-the-art for XCT and AM is examined in detail. XCT and AM are identified as having the potential to improve gold standards in both modelling and implant production, and in the conclusions of this review, primary barriers to the increased adoption of AM and XCT technologies are identified in reference to the main applications of XCT and AM technologies. The primary prohibitive factors generally relate to the cost of production across all of the examined applications, as well as the need for further clinical trials in surgical guidance and applications involving implantation.
Key words: X-ray computed tomography / additive manufacture / modelling
© A. Thompson et al., published by EDP Sciences, 2017
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
1 Introduction
Recent research regarding the combined use of X-ray computed tomography (XCT) and additive manufacturing (AM) in medicine is summarised in this review. The authors of this paper will focus specifically on application of XCT and AM in medicine and will not cover dental applications in great depth. Applications of XCT and AM use in dentistry are extensive and would easily form the subject of a separate review. Azari and Nikzad [1] examined the use of rapid prototyping in dentistry in 2009, summarising developments up until that point. This introduction details various AM process families as well as the basic principles of XCT. The contents of this review provide an overview of the historical and current state-of-the-art in the combined usage of XCT and AM in medicine. The review has been performed to provide an introduction to the medical applications of additive manufacturing.
1.1 Additive manufacturing processes
Additive manufacture is a process of joining materials to make objects from 3D model data, usually layer upon layer [2,3]. AM is now also known in the media as 3D printing, but the AM moniker is used in industry to more accurately define a wider range of manufacturing processes. This range of processes is divided into seven different process families defined by the American Society for Testing and Material (ASTM) [3]. Table 1 outlines the various process families.
AM holds a number of significant advantages when compared to subtractive or formative manufacturing (i.e. removal of material from a block to achieve a desired geometry and reformation of material into a desired geometry, respectively). One of these advantages is that AM allows easily for low volume production, as no additional tooling is required when producing new parts unlike in many subtractive and formative processes. This lack of tooling therefore aids in the production of highly personalised products such as medical implants. The other major advantage of AM is the freedom of design that is accessible using AM processes. As AM processes do not require machine tool access (unlike in subtractive manufacturing processes), AM allows for the production of previously unachievable complex geometries, particularly useful in, for example, mimicking porous biological structures such as bone [3].
As an emerging technology, AM techniques do, however, have a number of significant drawbacks when compared to comparable manufacturing processes. For example, in comparison to traditional machining or injection moulding, AM produced parts are usually limited by longer production times, poorer mechanical properties and poorer production accuracy [3]. There are a number of micro-additive processes that break this general rule, but these products are only capable of producing very small parts and so carry further restrictions [4]. It should also be noted that the pool of available materials available for use in AM processes is currently very small; AM research has not yet had the time required to develop the vast range of materials available to other manufacturing processes [3].
The primary AM processes used in medicine include SLA (for the production of models, moulds and surgical guides), SLS and FDM (for the production of models, moulds and end-use implants), and SLM and EBM (for the production of end-use implants). More recently, new material jetting technology has been used to create more complicated multi-colour and multi-material models for visualisation and surgical training, owing to the technology's ability to produce multi-material parts [5]. This review therefore primarily discusses these technologies. Figure 1 explains SLM, SLA and inkjetting diagrammatically, while SLS works in essentially the same manner as SLM and FDM replaces the material jetting printheads with a filament extruder.
1.2 The principles of XCT
XCT is a scanning technique used to produce three-dimensional (3D) representations of an object or patient, by taking many X-ray radiographs around a rotation axis and then reconstructing a 3D model using algorithms [6–8]. There have been five main XCT methods developed over time and the speed of data collection has increased with each generation of scanner [9]. The first generation [9] of XCT scanner used an X-ray pencil beam moved in a straight line opposite an X-ray detector to capture data about the object's density along each beam. The scanner was then moved a small amount around a circle until a 360° arc of data were acquired, covering a full slice in the xy plane. The source and detector were then moved incrementally in the z direction and the process was repeated. The first generation scanner was very slow which limited its capability for medical scanning, and so a second generation of scanner was quickly developed. The second generation scanner [9] operated similarly to the first, but used a fan of X-rays which translated across the patient. Although faster than the first, this second generation scanner also suffered from speeds too slow to allow viable scanning of moving objects. The third generation of XCT scanners was subsequently invented, and through improvements over time remains the most popular method of XCT scanning today. The third generation XCT scanners [9] use a two-dimensional (2D) X-ray fan that spans the whole object width at any point in time, with a one-dimensional (1D) detector array placed opposite the X-ray source to gain intensity data at each point along the fan. Later modifications to the third generation scanner resulted in the fourth generation scanner, which used a rotating X-ray source along with a static ring-shaped detector. The fourth generation scanners [9], however, suffer from high costs associated with the large number of detector elements as well as problems associated with scattered X-rays, and so despite the improved speed, fourth generation scanners remain less popular than their third generation counterparts. The most recent XCT scanners [9] use static sources and detectors, with an electron source used to change the position of the X-ray source, and are used in applications where very high speed scanning is desirable, such as in acquisition of cardiac data. One of the most important improvements to XCT technology came in the late 1980s [9] with the advent of helical (or “spiral”) scanning, which allowed XCT to move from a method of slice-orientated imaging to a method of full organ imaging. XCT scanners outside of medicine also commonly use a 3D cone of X-rays with a 2D detector [9]. In these cone-beam scanners, the cone beam of X-rays irradiates the entire object throughout the scan, thus greatly increasing the X-ray dosage to the object being scanned. Within the medical field, cone beam scanners are now extensively used in dentistry, as well as in intraoperatively for applications such as interventional radiology. Detector technology has changed over time, with early detectors using scintillation to detect X-ray photons while more modern detectors utilise element-based charge-coupled devices (CCDs) [9]. Figure 2 illustrates the various XCT scanner generations.
Following data capture, XCT data are reconstructing on a computer using the acquired intensities associated to each point in space. These intensity readings are acquired as a result of the summing individual linear attenuation coefficients along a linear path through the object being scanned. Using the linear intensity readings, the computer recreates slices of the object, which can then be combined to form a 3D reconstruction of the object [9]. The reconstruction can then be used simply for visualisation, or converted into an .STL (STereoLithography) file [10] for production using AM.
2 Historical overview of XCT and AM
Due to the volumetric nature of both XCT and AM technologies, the two technologies have experienced a strong relationship since shortly after the conception of stereolithography in 1986 [11], the original AM technology. As such, the first concurrent use of XCT and AM was three years later in 1990 by Mankovich et al. [12], who used SLA to a produce model of skull from XCT data (see Fig. 3). By today's standards, the resolution achieved on the model is very poor, but at the time, this model represented the first proof-of-concept study for production of anatomically correct models for planning and educational purposes. A similar study took place in 1992 [13] investigating the use of SLA in surgical planning, in which the authors highlight the advantages of SLA over CNC milling, achieving SLA resolution of 0.1 mm, far greater than the accuracy of milled models at the time. The authors do, however, note comparably long build times for SLA model production and, therefore, state that a speed increase could lead to SLA becoming a viable technique for surgical model production.
 |
Fig. 3 The first combined use of XCT and AM, producing an SLA skull model. Mankovitch et al. noted in the model the depiction of a cleft upper palate and the presence of imaging artefacts around the teeth in the XCT data, induced by the presence of incomplete attenuation profiles as a result of the patient's metal fillings [9]. Build problems were also noted in the B image relating to floating contours and the nature of the SLA process. Images reproduced from reference [12]. |
2.1 History pre-1995
As shown above, the initial use of XCT in AM was in a reverse engineering context, using XCT data to produce models, teaching aids and other non-functional parts. During the early days, XCT resolution was poor and AM technologies at that point were not capable of reproducing even those low resolution scans. As a result, rough interpretations similar to the skull shown in Figure 3 were the best achievable reproductions available. This section documents the shift from a reverse engineering based method of modelling to the accurate measurement tool that XCT has become more recently. Around the same time as the first produced skull, Bresina et al. [14] performed initial experiments using SLA for lost wax casting of bone replacements using the biocompatible material hydroxyapatite (HA). The study by Bresina et al. was the first occurrence of the use of XCT with AM for the production of implants, where XCT data were used in the design of scaffolds. The implants produced were brittle and so remained a long way from an implantable state. The authors also mentioned the direct use of SLS to process HA but commented on the poor part strength achieved. In 1994, Levy et al. [15] used XCT data from cadaveric temporal bone to generate SLS models from polycarbonate, which was the first documented use of SLS with XCT. The authors favourably compared SLS to SLA and milling, also mentioning direct SLS of HA for potential grafting applications. The authors concluded that SLS was capable of producing accurate models, noting several advantages including the capability for fine detail production and a wide range of materials. Further to this study, Lee and Barlow [16] presented initial results using SLS to process a polymer binder for HA parts. The green part was then fired to burn out the binder, which allowed infiltration by a calcium phosphate solution. Further firing was then performed to produce a craniofacial prosthesis from XCT data as a proof-of-concept. The authors noted acceptable reproduction of features, but also the presence of problems regarding the effects of surface area and micropores on green part strength, as well as part shrinkage incurred during firing operations. There were also two patent applications around this time discussing AM and XCT, regarding the production of industrial models and medical prostheses, the former detailing a powder bed fusion method, noting the use of XCT for object replication [17], while the latter focussed specifically on the rapid production of customised prostheses using XCT and SLS [18]. Around this time, owing to some of the aforementioned studies and a number of similar examples, the existence of both XCT and AM was starting to gain wider recognition. The editorial published by Ashley in Mechanical Engineering magazine [19] also provides insight into the very early use of XCT and AM; outlining the research and discussing AM processes. Ashley particularly discussed the potential that AM held in production of implants and prostheses, in addition to the technology's use in surgical planning.
2.2 History 1995–2005
The combined use of AM and XCT experienced rapid growth throughout the early 1990s, and as a result a large volume of research was published presenting an ever-expanding collection of AM technologies. AM in conjunction with XCT continued to be used during this time primarily for medical modelling, though usage was expanded during this period as the available imaging and production resolutions of XCT and AM improved. Owing to these improvements, XCT also began to be used as an inspection tool for industrially manufactured parts during this time [8]. Alongside the conception of the use of XCT as a part inspection tool, throughout the 1990s and early 2000s, there was continuous development of XCT and AM in the production of medical models. The first notable publication was in 1998, where D'Urso [20] registered a patent detailing a method for production of prostheses and anatomical models using XCT and SLA as well as a method for implanting those prostheses. Several papers were published through this period; for example, in the paper by Petzold et al. [21], the authors presented more advanced work into SLA for cranio-maxillofacial surgery, modelling skulls for use as implant forming templates. The authors noted that templates were usable during operations once sterilised and stated that higher quality and faster patient recovery were to be expected using rapid prototyped (RP) models. SLA was further used with XCT data during this time in various similar applications, including for modelling of dinosaur remains [22], cancellous bone [23], and castings for the production of durable pre-surgery models [24]. The authors of these papers note similar traits in the models they produced, generally observing enhanced visualisation in surgical training as well as improved pre-surgical planning of non-routine surgeries. In the paper by Bibb and Sisas [23], the authors contrasted models produced by SLA, SLS, 3D printing and FDM, citing the former as the preferable option due to maximal resolution and minimal porosity. In contrast to this comparison, in the same year, Berry et al. produced flexible silicone aortic aneurysms using XCT data to design castings made from SLS moulds. The authors stated that this method was preferable to a similar method used previously by Lermusiaux et al. [25], who produced SLA moulds, due to the reduced costs from the Berry method [26]. Another example of the use of XCT and AM in mould production involved a case study of an alloplastic cranial implant created using an FDM mould [27]. The authors concluded proof-of-concept as the resultant implant had good cosmetic results and noted that the operation time was significantly reduced as the implant required no intra-operative modification. The model was also noted to be useful for pre-surgical rehearsal. Winder and Bibb [28] used FDM, SLA and milling to produce medical models for maxillofacial, neurosurgical and orthopaedic applications. In this paper, the authors summarised model artefacts due to the process, including XCT data errors and tilt distortion, AM stair stepping, surface effects from support removal, metal image artefacts from fillings, movement artefacts from patients and image threshold artefacts from thin bone.
Concurrent to the research regarding the fabrication of medical models, several studies examined the direct production of implants, generally for tissue engineering purposes. As a group of technologies, AM is highly applicable to tissue scaffold production due to the ability of AM to produce highly porous lattice structures. When combined with patient XCT data, surgeons can design and produce mechanically tuneable and highly customised tissue scaffolds for direct implantation into patients. Three reviews were produced during this time that identified this technique as a viable method for production of scaffolds, as well as of prostheses and tissue models [29–31]. In 2003, Hollander et al. [32] performed preliminary studies using XCT with SLM for the purpose of directly replacing bone using TiAl6V4 implants. The authors observed that SLM implants showed increased biocompatibility in the form of greater metabolic activity of osteoblasts when compared to non-SLM control implants, which the authors attributed to the increased surface area of SLM implants. It was noted, however, that osteoblast coverage takes longer because of the increased surface roughness and as such represents a limitation towards adoption. It was, however, clear from this study that the proposed method warranted further exploration and a large amount of further work has been undertaken since this paper. This work included a feasibility study where Wehmöller et al. [33] used SLM for direct implant production using 100% stainless steel and titanium, and although the structures were not implanted, the authors concluded that the method was technically feasible. In a similar paper by Das et al. [34], the authors produced scaffolds using Nylon 6 via SLS, which is a biocompatible material, but noted problems with biocompatibility from unsintered powders. Also around this time, the first uses of XCT for inspection of AM parts were taking place. In the paper by Wang et al. [35], the authors performed XCT measurements of FDM scaffolds, proving the concept of XCT as a method of non-destructive evaluation (NDE) to measure internal morphology and porosity. Similarly, Williams et al. [36] performed XCT on polycaprolactone SLS scaffolds to create finite element analysis (FEA) models and to measure porosity, as well as to inspect scaffolds post-implantation (see Fig. 4). Conclusions stated that XCT imaging was adequate for FEA modelling (verified by mechanical testing) as well as in quantitative analysis of bone regeneration (verified by histological staining) and that the method showed great potential for skeletal tissue replacement.
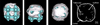 |
Fig. 4 Bottom, side and top views of surface rendered XCT data, showing bone formation around a render of the STL used to produce the implanted scaffold, as well as an individual XCT slice showing cortical shell and trabeculae within marrow spaces. Images reproduced from reference [36]. |
2.3 History 2005–2010
During the late 2000s, there were an ever-increasing number of studies investigating or using AM with XCT. The proportion of papers presented on medical modelling fell in comparison to those focussed on direct implant production or XCT inspection and metrology, but a large number of studies furthered research during this time, a selection of which can be seen in references [1,37–44]. This period showed a prevalence of the use of XCT in the design of various implants, summarised in a paper that detailed recent advances in production of tissue-engineering scaffolds [45]. In this study, Hollister converted XCT data to CAD data in order to design the bounds of a scaffold structure, contrasting various AM techniques for part production. Other similar studies discussing a variety of methods of additive scaffold production from XCT data can be found elsewhere [44,46–49]. In the papers by Mazzoli et al. [48] and Dinda et al. [49], the authors elaborate on AM production methods through microstructural and mechanical characterisation of manufactured scaffolds built from polyamide containing Al particles and Ti6Al4V respectively. These authors used scanning electron microscope (SEM) imaging, energy dispersive X-ray spectroscopy (EDX), X-ray diffraction (XRD) and various mechanical testing methods, to compare the designed implants to bone in which they could hypothetically be implanted. The authors concluded respectively that the materials used were highly useful in metallic appearance modelling (polyamide containing Al) and in direct tissue engineering applications (Ti6Al4V). Similarly, the paper by Faustini et al. [50] in 2008 demonstrated the feasibility of XCT and AM in production of customised orthoses, although the authors chose in this instance to base a series of SLS orthoses on XCT data of an existing carbon fibre model instead of designing their product in direct reference to patient data. The authors compared AM orthoses of different materials to the traditionally manufactured carbon fibre reference, concluding that the method presented considerable promise for the field.
As AM and XCT technologies have improved, XCT has been used increasingly as a tool for inspection and metrology, such as in two papers by Goodridge et al. [51,52] where the authors performed SLS on acrylic binder to produce glass-ceramic bone replacements. In the first paper [51], the authors mentioned the use of XCT in implant design, but also used XCT for non-metrological inspection of post-processed SLS parts showing potential for in vivo bone growth. In the latter paper [52], the authors implanted the bone replacements into rabbit tibiae, performing XCT scans on a weekly basis to show bone ingrowth. Numerous other cases of XCT as a visual inspection tool for AM parts, post-build and post-implantation, were also published around this time; examples of which can be found elsewhere [53–56]. In the paper by Saijo et al. [54], the authors presented the first human implantation of AM parts produced by binder jetting and based on patient XCT data, which achieved good biodegradability and osseoconductivity. Implants also achieved universal dimensional compatibility and partial union between host and artificial tissues, as shown by post-surgical XCT scans (see Fig. 5).
 |
Fig. 5 Left to right: pre-operative, immediately post-operative and six months post-operative XCT scans of first human AM implant. Images reproduced from reference [54]. |
2.4 History 2010–2014
As the field has moved forward, a lower proportion of studies relating to medical modelling have been published. A few notable studies have, however, been produced over the past five years. In a paper by Lethaus et al. [57], the authors used FDM to produce twenty patient mandible models from XCT data, which were then used to pre-bend reconstruction plates prior to surgery. Results showed substantial time saved during operations due to plate bending no longer being required during surgery. Similarly, Appleby et al. [58] replicated the remains of Richard III (found recently buried beneath a Leicester car park) from XCT data using SLS. The AM recreation was then used to inform historians about the king's spinal defect and has since been exhibited for educational purposes. This period also saw a rise in the implantation of AM implants, such as in the paper by Figliuzzi et al. [59], where the authors produced Ti6Al4V dental root-analogue implants from XCT data and implanted them immediately after root extraction. Follow-up XCT after one year showed near perfect functional and aesthetic integration, with enhanced osseointegration due to the porous surface of the additive implant. Following this, Mangano et al. [60] performed a clinical study involving the implantation of custom Ti implants designed in reference to XCT data, which showed retained functionality two years following implantation. The authors also noted that their method presented a reduction in treatment complexity compared to other options. In their 2012 review, Seol et al. [61] highlighted different AM technologies for tissue engineering and discusses the use of XCT for this purpose, while Mazzoli [62] highlighted a number of further examples of implantation in her 2013 review. Mazzoli also summarised the general biomedical implications of AM, noting the use of AM in production of drug delivery devices and biodegradable scaffolds.
3 XCT and AM in medicine today
3.1 Use for medical modelling
During the past twelve months, a large array of publications has continued to be produced using XCT with a variety of AM techniques to produce medical models for a diverse range of purposes [63–85]. Many of these studies used older AM techniques for the modelling of novel but relatively routine medical applications and so will not be detailed here, although a few studies from this subset are worth noting for their particular innovation or use of more advanced AM technologies. For example, in two papers by Mayer et al. [67] and Bache et al. [78], the authors produced X-ray dosimeters for different purposes. Mayer et al. used XCT with inkjetting to produce a multimaterial thorax phantom, which when combined with dosimetry allowed measurement of X-ray dosage to a tumour within the model thorax. Bache et al. similarly used XCT to produce FDM moulds for rodent-morphic dosimeters, to be used as a tool in preclinical microstereotactic-body-radiation-therapy. The multi-material approach to phantom production used by Mayer et al. was echoed in the paper by Kiarashi et al. [71], where the authors developed two breast phantoms based on XCT data and produced via inkjetting. One of the phantoms was made using two materials representing fibroglandular and adipose tissues respectively, while the other was produced from a single material to represent fibroglandular tissue and skin and then filled with a second material similar to adipose tissue. Mammography was then performed on each of the phantoms, which showed realistic breast anatomy and proved the phantoms' success. Further to this, Igami et al. [63] and Isotani [72] drew attention respectively to the creation of multi-colour models of a single-material liver produced via SLA (later coloured with a dye) and a multi-material kidney produced via inkjetting; both using CAD models extracted from XCT data and used as an aid to surgical approach design. Kondo et al. [69] and Kenngott et al. [80] also produced multi-coloured, single-material models through the use of binder jetting with XCT. The former authors produced models of unruptured cerebral aneurysms for neurosurgical simulation, while the latter produced an anatomically correct haptic torso phantom on an open source platform for surgical evaluation and training (see Fig. 6).
As the use of models has increased in general day-to-day medical practise, a number of studies have examined various metrics assessing long-term usefulness of the technology in order to continue the process of universal adoption. Several of the aforementioned studies examine and conclude generally positive findings: medical models of various types are useful in pre-operative planning of complicated surgery, which reduces operation time. Other conclusions included the fact that medical modelling increases and enhances student understanding in training and patient understanding in consultation [65,75–77,79,81,83], and it can be concluded from these studies that medical models have proven increasingly useful over time for a variety of medical applications. From the studies examined in this paper, it is clear that the development in medical modelling is most notably in the area of materials and processes that allow the production of multi-colour models. XCT is of most use in modelling of bones and teeth, as well as of blood vessels (via contrast XCT angiography). It should, however, be noted that the improved soft tissue imaging contrast offered by magnetic resonance imaging (MRI) [86], as well as the lack of X-ray dose to patients, leads the authors to believe that the MRI is of more use in medical modelling of soft tissues. Further discussion of recent XCT and AM usage in medical modelling can be found in reference [87].
 |
Fig. 6 Top left: dyed SLA liver [63], top right: inkjetted kidney [72], centre: binder jetted cerebral aneurysm [69], bottom: binder jetted torso phantom [80]. Images reproduced from references outlined above. |
3.2 Use for surgical guidance
The combined use of XCT and AM technologies is also now becoming more prevalent in the field of surgical guidance in production of patient specific guides to ensure correct placement of surgical screws or to inform surgeons of correct drill-hole angle and placement [88–95]. These guides are very commonly used in cranio-maxillofacial surgery, particularly in the placement of AM dental implants primarily through the use of SLA with XCT. Reyes et al. [92], however, compared the production of SLA guides to those produced by inkjetting, using CAD data adapted from either patient XCT data or optical scans of dental casts. Reyes et al. concluded in this case that the most accurate guides for this application were produced by inkjetting of optical scan data. By contrast, Widmann et al. [91] fused optical scan and XCT data together to form CAD models, and then produced the resulting models using SLA. Takemoto et al. [93] developed patient-specific pedicle screw placement templates, which showed high positional accuracy success rates when evaluated visually, intra- and post-operatively, for the former and using XCT for the latter. Huang et al. [94] similarly noted adequate positional accuracy of implants placed using SLA guides, concluding that the method successfully facilitated the diagnosis, planning and treatment of the examined dental problems. In another application, Laycock et al. [96] used AM with XCT to produce binder jetted immobilisation moulds for head and neck radiotherapy, in order to replace traditionally poor fitting moulds.
The use of XCT with AM for the production of surgical guides represents a particularly interesting application of these combined technologies, as surgical guides are commonly used for surgeries performed on internal tissues, where high precision, accurate volumetric scanning and manufacture is an obvious requirement. Future developments in the field will likely result in an increase of precision and accuracy in scanning and manufacturing, so as to improve the fit between guides and the patient, and ultimately the quality of the surgical output. In keeping with these likely developments, it is worth noting that as XCT has increased in use as a metrological tool [8], a number of medical authors have similarly adopted the technology beyond its ability to recreate geometries and as a medical inspection device. Examples of this include the post-operative assessment of implant positional and angular deviation compared to the intended positioning [90], and the comparison between patient XCT data and XCT scans of AM models, through calculation of the root mean square error of surface variations [80]. Also of note as an aside to this section, Singh et al. [97] recently presented a design for an AM training box to account for a lack of training objects in the field of endoscopic neurosurgery. The training box was designed in reference to XCT dimensional measurements of a patient's skull in order to build the training device to a typical head size. Further metrological use of XCT in medicine is discussed in reference [8].
Similarly in medical modelling applications, a number of studies have examined the long-term effects of using AM surgical guides. As concluded regarding medical models, in surgical guidance the evidence is also generally in favour of AM technology, where Sakai et al. [85] and Orentlicher et al. [88] both note good cumulative survival rates of dental implants placed using XCT-based SLA guides. These authors also noted that XCT-guided implantation increases safety compared to freehand techniques, with the caveat that aesthetic results of the implants were comparatively poor. It is clear from these studies, as well as the general proliferation of the combined use of XCT and AM in medicine, that the use in surgical guidance of these technologies is a highly useful practise that will likely continue to expand as awareness increases and the prohibitive cost of AM machines decreases over time.
3.3 Use for endoprosthetics and orthotics
Another recent example of AM used with XCT lies in the production of endoprosthetics and orthotics. Leordean et al. [98], for example, proposed the production of a customised endoprosthesis, designed in reference to patient XCT data and FEA simulations of ordinary human activity based upon the XCT data. Liacouras et al. [99] similarly used XCT with AM to fabricate an auricular prosthesis from mirrored XCT data of a patient's ear. The authors in this case used binder jetting to produce a mould from patient data, and then used to produce the prosthetic device. The authors have since produced three more prostheses using the same method and have reported high levels of patient satisfaction and a reduced cycle time compared to traditional moulding methods, with good correspondence between prosthetic and soft tissue geometries. A comprehensive review of the use of AM for production of orthoses and prostheses was recently published by Chen et al. [100], in which the authors discuss the use of XCT for the purpose of data capture among other data capture technologies. The authors in the case conclude the usefulness of AM in orthotic and prosthetic production, but note a lack of an appropriate clinical and design interface, uneconomic throughput and material cost, and material strength as the current primary barriers to increased adoption.
3.4 Use for implants (stand-alone)
As previously highlighted, a large number of studies developing patient specific human implants have been published since the early 1990s. These studies have continued into the very recent past, but the focus has shifted from proof-of-concept to verification of implants, including dimensional measurements and tolerancing. Similarly, Otawa et al. [101] published their work on accuracy verification of guided bone regeneration membranes designed in reference to XCT data, using a micrometer for dimensional measurements and the Archimedes principle to measure porosity. The produced specimens were within the ISO 2768-1 [102] tolerance and the authors deemed the method suitable for clinical application. In the growing field of bioprinting (i.e. the formation of 3D tissues through direct printing of functional, viable cells [103]), XCT data are also now being used to inform designs to produce more complex structures. This field in particular represents a novel and interesting use of AM with XCT, which will likely continue to produce patient specific complete organ implants; further examples of XCT and AM usage in tissue engineering are covered in two recent reviews [104,105].
AM production and implantation of basic personalised implants based on XCT data are now commonplace, and reflecting this, a wide array of studies involving implantation have been published over the past year as the technology has become better understood [106–119]. Clinical usage of metallic implants produced by AM in particular is now becoming common, specifically in maxillofacial and orthopaedic applications, though a number of issues remain preventing further adoption. In terms of polymeric implants, problems with material certification are currently preventing commercialisation, but the available literature implies that a wealth of potential applications exists. A number of studies over the past twelve months have been published involving implantation into animals using a variety of AM technologies for various applications. Xu et al. [106] produced artificial goat femurs using XCT with FDM of a hydroxyapatite/polycaprolactone (HA/PCL) composite, showing good biocompatibility and bone-analogous load bearing performance in vitro and in vivo, concluding that extension to human patients was viable. Similarly, van Uden et al. [114] used XCT data with FDM to create PCL intervertebral disk scaffolds with mechanical properties similar to native tissue. XCT was then performed pre- and post-operatively following implantation into rabbits to analyse porosity and compare implants to the native tissue; in this instance finding the compressive stiffness to be greater than human native tissue. Li et al. [110] sought to prevent long-term complications in dogs following pneumonectomy through AM production of XCT based prosthetic implants, and post-operative XCT scans of the implants at three-month intervals for one year showed decreased morbidity compared to animals without implants. Haefeli et al. [119] implanted SLM Ti implants into cadaveric specimens, using XCT to assess achieved precision through deviation of surfaces between reconstructed scaphoids and their virtual counterparts. The results showed good precision in only half of the ten cases, but the authors attributed problems to template design and stated that they could be avoided by improved pre-operative planning, shown through presentation of a clinical case. XCT was then performed three months post-operatively and showed successful bony fusion of the scaphoid.
As demonstrated in the latter study by Haefeli et al. [119], XCT based implants are now increasingly used in humans, and further examples of implantation are presented elsewhere [107–109,111,115,118]. A particularly common application remains in cranio-maxillofacial surgery, and Jardini et al. [107], Radovan et al. [108] and Cho et al. [118] present case studies involving the implantation of devices to replace various skull defects, produced using metallic powder bed fusion with XCT data. These authors all concluded successful results of shorter surgical times, as well as higher accuracy implant production compared to traditional production methods, confirmed using post-operative XCT. Radovan et al. [108] also investigated implant accuracy in more detail, overlaying CAD data onto scanned data to produce a variance map. The authors imposed a tolerance of 0.3 mm and showing that the majority of the implant was within tolerance with some local deviations, which the authors attributed to the scanning technology and the position of the implant during the scanning process. It should be noted that despite the implant falling outside of the tolerance, the authors made the decision that the implant was sufficiently accurate and so successfully implanted it into the patient regardless of this problem.
Although they remain largely in the experimental laboratory and are not yet in widespread clinical use, ceramic implants designed in reference to XCT data also hold potential for future clinical exploitation, and a recent review by Vorndran et al. [120] discussed these at length. The authors in this case concluded that production of ceramic implants in relation to patient data is currently possible, and that drug modification of these implants can be achieved, further noting the future potential for direct cell-seeding of patient specific implants for bone regeneration. The main current barriers noted were the requirement for a clean and sterile manufacturing process, as well as difficulties with repeatability and reproducibility of implants.
3.5 Use for implants (scaffolds)
In addition to the production of personalised implants, AM is increasingly being used for the production of tissue scaffolds for implantation. Lueders et al. [121], for example, recently published their initial results in the production of customised heart valve scaffolds from XCT data, using bioresorbable polymers and seeding valves with vascular cells, with the overall intention of producing a fully bioresorbable customised heart valve. Rasperini et al. [111] recently presented a periodontitis case in which bioresorbable HA/PCL processed via SLS with XCT data was used to produce a scaffold for repair of an osseous defect. Postoperative examination at two, six and twelve months showed that the treated site remained intact for the duration of this time, although it failed shortly following the twelve-month point and was removed. The authors do conclude, however, that despite eventual failure of the implant, the method warranted further study in the field of personalised oral regenerative medicine. Further information respectively regarding the use of AM for tissue engineering and AM for oral and maxillofacial surgery and the associated challenges faced in these fields is available in the recent reviews by Shirazi et al. [112] and Farré-Guasch et al. [113]. It is clear from these recent studies, as well as others discussed earlier in this review, that XCT and AM represent an excellent opportunity for various aspects of medicine to evolve and improve to meet the higher standards offered by XCT and AM. XCT and AM technologies primarily offer faster surgeries with greater long-term success rates, due to the patient specific accuracies offered by highly personalised AM implants. A wide array of studies have been conducted into AM fabrication of scaffolds, examining surface topography and chemistry, as well as the effects of pore size and lattice construction, on how scaffolds behave in a medical context. The recent review performed by Wang et al. [122] examines these studies in depth, in addition to a discussion of AM fabrication of orthopaedic implants, both in the context of topology optimisation in implant design. The authors in this case conclude that AM provides an excellent opportunity for implant production, and note a number of challenges relating to the requirement for a comprehensive atlas of the mechanical properties of human bones, as well as in regards to further development of topology optimisation algorithms and lattice design. Wang et al. finally make reference to a requirement for further in vivo testing of topology optimised implants and development of novel alloying and post-processing systems for improving mechanical and biological properties.
4 Conclusions and future research
The above discussion of current studies represents the state-of-the-art use of XCT in AM. It was clear from the available literature that research utilising XCT and AM falls into five primary areas, although the number of unique applications is substantially in excess of this. These primary areas have been discussed in detail and it is possible to draw specific conclusions regarding each of the applications within each research area.
In medicine, XCT is now commonly used with AM in the following primary applications: the production of anatomical models, surgical guides, endoprosthetics and orthotics, stand-alone implants and scaffold implants. These applications rely on the principles of reverse engineering, using patient XCT data to inform the design process. AM has been widely acknowledged as the most appropriate manufacturing method of production of customised products, due to the lack of associated tooling required and the ability to produce highly complex geometries. These advantages make AM invaluable in tissue engineering applications, where the production of micro-scale lattice structures is an intrinsic requirement.
Focussing on the use of XCT and AM in medical model production, the consensus is that the technologies are successful in sufficiently accurate organ reproduction and as a result, surgical times have been reduced in many complex surgeries. Models have also been used in education of doctors and patients alike, and several of the aforementioned studies have concluded the high degree of their usefulness in this application. It can be stated, therefore, that the use of XCT and AM for medical modelling is now a well-established practice, although many researchers have acknowledged a lack of adoption. The primary barrier to adoption that is noted by most authors is the high relative cost of model production. In a field where budgets are often limited, it is easy to understand how justifying the purchase of a costly piece of equipment, only useful in a small number of complex cases, is difficult, although some authors also discuss the lack of professional awareness as an equally prohibitive barrier.
Studies of XCT-based AM surgical guides showed that the production of sufficiently accurate products was possible, and regarding recent studies, generally speaking very good correlation between these products and patients' internal geometry was achieved. XCT and AM hold excellent potential for development in surgical guidance, offering a novel and greatly improved method of implant placement when compared to traditional surgical guidance techniques. The main issue preventing further adoption of these technologies in the field of surgical guidance is the cost of guide production, as the high costs commonly associated with AM prevent many in the medical field from utilising these novel methods of guide manufacture.
Regarding the use of XCT and AM in production of endoprosthetics and orthotics, it should be noted that while XCT represents an interesting solution for data capture of internal patient geometry for endoprosthetic production, orthotic structures are more commonly produced in reference to data captured by optical scanning methods, so as to remove the radiation dose to the patient [100]. As orthotic devices do not usually require internal information and are produced to fit a patient's external geometry, this approach is generally adequate.
The primary barrier identified in the case of both standalone and scaffold implant production was usually an identification of the requirement for in vivo human testing, as the amount of implants that have actually been implanted into humans is much smaller than the number of studies concluding the successful production of implants. Despite this, a small number of implants have been implanted, and study of these has generally showed results similar to those regarding model production. Outcomes of these papers often discussed resulting shorter surgical times and improved fits with respect to conventional implants, but increased production costs. Over time, the use of post-operative XCT in examination of implant positioning has improved as XCT has become more established as a metrological tool, from an approximate method of visual confirmation, to a rigorous surgical verification tool used with respect to tolerancing. This verification is, however, only used by a small proportion of authors and more widespread adoption of post-operative metrology would represent an increase in good practice, likely resulting in further increased implant success. Future research in medical XCT for AM should work towards overcoming these barriers, tying into general AM research regarding cost reduction and the promotion of good practice through verification, particularly in cases where parts are designed for implantation.
A final point of note to this study is that, although a full discussion of the use of MRI and AM in medicine is out of the scope of this review, it is worth briefly discussing the use of XCT versus MRI for generation of the patient data used for AM in medicine. It is well known that MRI has a number of advantages over XCT, relating to the nature of MRI as a technology [86]. Unlike MRI, XCT inherently provides a high dose of ionising radiation to the patient, and although improvements in clinical XCT over time have reduced the dose [9], it is intrinsic to XCT technology and therefore impossible to reduce that dose to zero. MRI as a technology is also more readily available and able to achieve much better contrast between soft tissues when compared to XCT, and so similarly represents an interesting method of data capture for production of AM parts in medicine. However, while MRI may well be in the process of superseding XCT in many areas of data capture medicine, imaging of skeletal morphology remains a core competency of XCT over MRI [86]. When compared to XCT, MRI particularly fails in imaging of bone tissue, as bone gives a low signal in MRI scans and the contrast between bone and other tissues is often low. Because this contrast is frequently poor, segmentation of bone tissue is commonly therefore difficult to achieve with the accuracy required by the applications outlined in this review. For this reason, the authors perceive a rich future in the combined use of XCT with AM for the production of many of the parts for the aforementioned applications. The authors therefore expect that as the price of AM parts reduces over time, adoption of XCT and AM technologies in medicine will increase, therefore allowing patients to reap the associated benefits.
In summary, XCT and AM have gained increasing prevalence within medicine for a number of applications. A large volume of research into both areas has been performed over the past three decades and the technologies are now becoming relatively well established, though there remain the following primary barriers to increased adoption of XCT and AM technologies within medicine:
-
in medical modelling: the cost of model production remains the most prohibitive factor in this area and removal of this barrier should naturally follow with the decreasing costs of AM technologies over time;
-
in surgical guidance, as well as stand-alone and scaffold based implant production: further clinical trials of customised AM implants and guides based on XCT data are required, allowing widespread use of this technology as a new, higher standard for implants and guides;
-
in endoprosthetics and orthotics production: AM represents a promising tool for part production, but due to the nature of endoprosthetics and orthotics, it is more common to use optical surface scanning for data capture, though XCT may be useful in some applications;
-
in production of stand-alone and scaffold based implants: AM and XCT remain hindered by a lack of clinical trials, as well as associated production costs, but initial results in implantation of AM parts are positive and these technologies represent an interesting future for implant production.
XCT and AM were first jointly used as a reverse engineering tool for low quality models in the 1990s, but the technology available has progressed greatly since those initial experiments. XCT is now used extensively in conjunction with AM for high accuracy production of tactile models and highly customisable implants, which have the potential to present a new gold standard in reconstructive surgery. The combined XCT and AM technologies represent an excellent opportunity in the coming years for a general advancement of standards within medical practice.
5 Implications and influences
The research contained in this contribution provides an overview of the combined use of AM and XCT in a medical context, and serves to inform those new to these areas of the history of and the state-of-the-art in the field. This work provides a basic overview of the topic and will influence future work through identification of the primary barriers to increased adoption of these technologies within medicine.
Acknowledgments
The authors would like to thank the Engineering and Physical Sciences Research Council (EPSRC Grants EP/M008983/1 and EP/L01534X/1) and 3T RPD Ltd. for funding this work.
References
- A. Azari, S. Nikzad, The evolution of rapid prototyping in dentistry: a review, Rapid Prototyp. J. 15, 216–225 (2009) [Google Scholar]
- ASTM F2792-12a, Standard Terminology for Additive Manufacturing Technologies (ASTM International, West Conshohocken, PA, 2012) [Google Scholar]
- I. Gibson, D. Rosen, B. Stucker, Additive Manufacturing Technologies: 3D Printing, Rapid Prototyping, and Direct Digital Manufacturing (Springer, New York, NY, 2014) [Google Scholar]
- M. Vaezi, H. Seitz, S. Yang, A review on 3D micro-additive manufacturing technologies, Int. J. Adv. Manuf. Technol. 67, 1721–1754 (2013) [Google Scholar]
- H. Wijshoff, The dynamics of the piezo inkjet printhead operation, Phys. Rep. 491, 77–177 (2010) [Google Scholar]
- J.-P. Kruth, M. Bartscher, S. Carmignato, R. Schmitt, L. De Chiffre, A. Weckenmann, Computed tomography for dimensional metrology, CIRP Ann. Manuf. Technol. 60, 821–842 (2011) [Google Scholar]
- L. De Chiffre, S. Carmignato, J.-P. Kruth, R. Schmitt, A. Weckenmann, Industrial applications of computed tomography, CIRP Ann. Manuf. Technol. 63, 655–677 (2014) [Google Scholar]
- A. Thompson, I. Maskery, R.K. Leach, X-ray computed tomography for additive manufacturing: a review, Meas. Sci. Technol. 27, 072001 (2016) [Google Scholar]
- J. Hsieh, Computed Tomography: Principles, Design, Artifacts, and Recent Advances (SPIE Press, Bellingham, WA, 2009) [Google Scholar]
- L. Roscoe, Stereolithography Interface Specification (3D Systems Inc., Rock Hill, SC, USA, 1988) [Google Scholar]
- C.W. Hull, Apparatus for Production of Three-Dimensional Objects by Stereolithography, US 4575330 A, 1986 [Google Scholar]
- N.J. Mankovich, A.M. Cheeseman, N.G. Stoker, The display of three-dimensional anatomy with stereolithographic models, J. Digit. Imaging 3, 200–203 (1990) [Google Scholar]
- H. Klein, W. Schneider, G. Alzen, E. Voy, R. Günther, Pediatric craniofacial surgery: comparison of milling and stereolithography for 3D model manufacturing, Pediatr. Radiol. 22, 458–460 (1992) [CrossRef] [PubMed] [Google Scholar]
- S. Bresina, M. Vannier, S. Tepic, S. Perren, Automated production of custom bone replacements, in Proceedings of the 12th Annual internation conferenence of the IEEE Engineering in Medicine and Biology Society (EMBS) (IEEE, Philadelphia, PA, 1990), pp. 385–386 [Google Scholar]
- R.A. Levy, S. Guduri, R.H. Crawford, Preliminary experience with selective laser sintering models of the human temporal bone, Am. J. Neuroradiol. 15, 473–477 (1994) [Google Scholar]
- G. Lee, J. Barlow, Selective laser sintering of calcium phosphate powders, in Solid Freeform Fabrication Symposium Proceedings (University of Texas Austin, Austin, TX, 1994), pp. 191–197 [Google Scholar]
- I. Pomerantz, J. Cohen-Sabban, A. Bieber, J. Kamir, M. Katz, M. Nagler, Three Dimensional Modelling Apparatus, US 5031120 A, 1991 [Google Scholar]
- D.J. Fink, S.T. DiNovo, T.J. Ward, Rapid, Customized Bone Prosthesis, US 5370692 A, 1994 [Google Scholar]
- S. Ashley, Rapid prototyping for artificial body parts, Mech. Eng. 115, 50–53 (1993) [Google Scholar]
- P.S. D'Urso, Stereolithographic Anatomical Modelling Process, US 5741215 A, 1998 [Google Scholar]
- R. Petzold, H.-F. Zeilhofer, W. Kalender, Rapid prototyping technology in medicine—basics and applications, Comput. Med. Imaging Graph. 23, 277–284 (1999) [CrossRef] [PubMed] [Google Scholar]
- P. D'Urso, R. Thompson, W. Earwaker, Stereolithographic (SL) biomodelling in palaeontology: a technical note, Rapid Prototyp. J. 6, 212–216 (2000) [Google Scholar]
- R. Bibb, G. Sisias, Bone structure models using stereolithography: a technical note, Rapid Prototyp. J. 8, 25–29 (2002) [Google Scholar]
- O.L. Harrysson, D.R. Cormier, D.J. Marcellin-Little, K. Jajal, Rapid prototyping for treatment of canine limb deformities, Rapid Prototyp. J. 9, 37–42 (2003) [Google Scholar]
- P. Lermusiaux, C. Leroux, J.C. Tasse, L. Castellani, R. Martinez, Aortic aneurysm: construction of a life-size model by rapid prototyping, Ann. Vasc. Surg. 15, 131–135 (2001) [CrossRef] [PubMed] [Google Scholar]
- E. Berry, A. Marsden, K. Dalgarno, D. Kessel, D. Scott, Flexible tubular replicas of abdominal aortic aneurysms, Proc. Inst. Mech. Eng. H: J. Eng. Med. 216, 211–214 (2002) [CrossRef] [Google Scholar]
- S. Gopakumar, RP in medicine: a case study in cranial reconstructive surgery, Rapid Prototyp. J. 10, 207–211 (2004) [Google Scholar]
- J. Winder, R. Bibb, Medical rapid prototyping technologies: state of the art and current limitations for application in oral and maxillofacial surgery, J. Oral Maxillofac. Surg. 63, 1006–1015 (2005) [Google Scholar]
- D.W. Hutmacher, Scaffolds in tissue engineering bone and cartilage, Biomaterials 21, 2529–2543 (2000) [CrossRef] [PubMed] [Google Scholar]
- W. Sun, P. Lal, Recent development on computer aided tissue engineering—a review, Comput. Methods Programs Biomed. 67, 85–103 (2002) [CrossRef] [PubMed] [Google Scholar]
- D.W. Hutmacher, M. Sittinger, M.V. Risbud, Scaffold-based tissue engineering: rationale for computer-aided design and solid free-form fabrication systems, Trends Biotechnol. 22, 354–362 (2004) [CrossRef] [PubMed] [Google Scholar]
- D.A. Hollander, T. Wirtz, M. von Walter, R. Linker, A. Schultheis, O. Paar, Development of individual three-dimensional bone substitutes using “selective laser melting”, Eur. J. Trauma 29, 228–234 (2003) [CrossRef] [Google Scholar]
- M. Wehmöller, P. Warnke, C. Zilian, H. Eufinger, Implant design and production—a new approach by selective laser melting, in International Congress Series (Elsevier, Berlin, 2005), pp. 690–695 [Google Scholar]
- S. Das, S.J. Hollister, C. Flanagan, A. Adewunmi, K. Bark, C. Chen et al., Freeform fabrication of nylon-6 tissue engineering scaffolds, Rapid Prototyp. J. 9, 43–49 (2003) [Google Scholar]
- F. Wang, L. Shor, A. Darling, S. Khalil, W. Sun, S. Güçeri et al., Precision extruding deposition and characterization of cellular poly-ε-caprolactone tissue scaffolds, Rapid Prototyp. J. 10, 42–49 (2004) [Google Scholar]
- J.M. Williams, A. Adewunmi, R.M. Schek, C.L. Flanagan, P.H. Krebsbach, S.E. Feinberg et al., Bone tissue engineering using polycaprolactone scaffolds fabricated via selective laser sintering, Biomaterials 26, 4817–4827 (2005) [CrossRef] [PubMed] [Google Scholar]
- D.A. Hollander, M. Von Walter, T. Wirtz, R. Sellei, B. Schmidt-Rohlfing, O. Paar et al., Structural, mechanical and in vitro characterization of individually structured Ti-6Al-4V produced by direct laser forming, Biomaterials 27, 955–963 (2006) [CrossRef] [PubMed] [Google Scholar]
- M. Suzuki, A. Hagiwara, Y. Ogawa, H. Ono, Rapid-prototyped temporal bone and inner-ear models replicated by adjusting computed tomography thresholds, J. Laryngol. Otol. 121, 1025–1028 (2007) [CrossRef] [PubMed] [Google Scholar]
- J.A. Henry, G. O'Sullivan, A.S. Pandit, Using computed tomography scans to develop an ex-vivo gastric model, World J. Gastroenterol. 13, 1372–1377 (2007) [CrossRef] [PubMed] [Google Scholar]
- E.K. Sannomiya, J.V.L. Silva, A.A. Brito, D.M. Saez, F. Angelieri, G. da Silva Dalben, Surgical planning for resection of an ameloblastoma and reconstruction of the mandible using a selective laser sintering 3D biomodel, Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 106, e36–e40 (2008) [Google Scholar]
- S. Singare, Q. Lian, W. Ping Wang, J. Wang, Y. Liu, D. Li et al., Rapid prototyping assisted surgery planning and custom implant design, Rapid Prototyp. J. 15, 19–23 (2009) [Google Scholar]
- R. Bibb, J. Winder, A review of the issues surrounding three-dimensional computed tomography for medical modelling using rapid prototyping techniques, Radiography 16, 78–83 (2010) [Google Scholar]
- M. Wanibuchi, M. Ohtaki, T. Fukushima, A.H. Friedman, K. Houkin, Skull base training and education using an artificial skull model created by selective laser sintering, Acta Neurochir. 152, 1055–1060 (2010) [CrossRef] [Google Scholar]
- I. Gibson, L. Cheung, S. Chow, W. Cheung, S. Beh, M. Savalani et al., The use of rapid prototyping to assist medical applications, Rapid Prototyp. J. 12, 53–58 (2006) [Google Scholar]
- S.J. Hollister, Porous scaffold design for tissue engineering, Nat. Mater. 4, 518–524 (2005) [CrossRef] [PubMed] [Google Scholar]
- B.V. Krishna, S. Bose, A. Bandyopadhyay, Low stiffness porous Ti structures for load-bearing implants, Acta Biomater. 3, 997–1006 (2007) [Google Scholar]
- L. Murr, S. Gaytan, F. Medina, H. Lopez, E. Martinez, B. Machado et al., Next-generation biomedical implants using additive manufacturing of complex, cellular and functional mesh arrays, Philos. Trans. R. Soc. A 368, 1999–2032 (2010) [CrossRef] [Google Scholar]
- A. Mazzoli, G. Moriconi, M.G. Pauri, Characterization of an aluminum-filled polyamide powder for applications in selective laser sintering, Mater. Des. 28, 993–1000 (2007) [Google Scholar]
- G. Dinda, L. Song, J. Mazumder, Fabrication of Ti-6Al-4V scaffolds by direct metal deposition, Metall. Mater. Trans. A 39, 2914–2922 (2008) [CrossRef] [Google Scholar]
- M.C. Faustini, R.R. Neptune, R.H. Crawford, S.J. Stanhope, Manufacture of passive dynamic ankle-foot orthoses using selective laser sintering, IEEE Trans. Bio-Med. Eng. 55, 784–790 (2008) [CrossRef] [Google Scholar]
- R. Goodridge, K. Dalgarno, D. Wood, Indirect selective laser sintering of an apatite-mullite glass-ceramic for potential use in bone replacement applications, Proc. Inst. Mech. Eng. H: J. Eng. Med. 220, 57–68 (2006) [CrossRef] [Google Scholar]
- R.D. Goodridge, D.J. Wood, C. Ohtsuki, K.W. Dalgarno, Biological evaluation of an apatite-mullite glass-ceramic produced via selective laser sintering, Acta Biomater. 3, 221–231 (2007) [Google Scholar]
- C.Y. Lin, T. Wirtz, F. LaMarca, S.J. Hollister, Structural and mechanical evaluations of a topology optimized titanium interbody fusion cage fabricated by selective laser melting process, J. Biomed. Mater. Res. A 83, 272–279 (2007) [CrossRef] [PubMed] [Google Scholar]
- H. Saijo, K. Igawa, Y. Kanno, Y. Mori, K. Kondo, K. Shimizu et al., Maxillofacial reconstruction using custom-made artificial bones fabricated by inkjet printing technology, J. Artif. Organs 12, 200–205 (2009) [CrossRef] [PubMed] [Google Scholar]
- L. Moroni, G. Poort, F. Van Keulen, J. De Wijn, C. Van Blitterswijk, Dynamic mechanical properties of 3D fiber-deposited PEOT/PBT scaffolds: an experimental and numerical analysis, J. Biomed. Mater. Res. A 78, 605–614 (2006) [CrossRef] [PubMed] [Google Scholar]
- M. Smith, C. Flanagan, J. Kemppainen, J. Sack, H. Chung, S. Das et al., Computed tomography-based tissue-engineered scaffolds in craniomaxillofacial surgery, Int. J. Med. Robot. Comput. Assist. Surg. 3, 207–216 (2007) [CrossRef] [Google Scholar]
- B. Lethaus, L. Poort, R. Böckmann, R. Smeets, R. Tolba, P. Kessler, Additive manufacturing for microvascular reconstruction of the mandible in 20 patients, J. Craniomaxillofac. Surg. 40, 43–46 (2012) [CrossRef] [PubMed] [Google Scholar]
- J. Appleby, P.D. Mitchell, C. Robinson, A. Brough, G. Rutty, R.A. Harris et al., The scoliosis of Richard III, last Plantagenet King of England: diagnosis and clinical significance, Lancet 383, 1944 (2014) [CrossRef] [PubMed] [Google Scholar]
- M. Figliuzzi, F. Mangano, C. Mangano, A novel root analogue dental implant using CT scan and CAD/CAM: selective laser melting technology, Int. J. Oral Maxillofac. Surg. 41, 858–862 (2012) [CrossRef] [PubMed] [Google Scholar]
- F. Mangano, M. Bazzoli, L. Tettamanti, D. Farronato, M. Maineri, A. Macchi et al., Custom-made, selective laser sintering (SLS) blade implants as a non-conventional solution for the prosthetic rehabilitation of extremely atrophied posterior mandible, Lasers Med. Sci. 28, 1241–1247 (2013) [CrossRef] [PubMed] [Google Scholar]
- Y.-J. Seol, T.-Y. Kang, D.-W. Cho, Solid freeform fabrication technology applied to tissue engineering with various biomaterials, Soft Matter 8, 1730–1735 (2012) [Google Scholar]
- A. Mazzoli, Selective laser sintering in biomedical engineering, Med. Biol. Eng. Comput. 51, 245–256 (2013) [Google Scholar]
- T. Igami, Y. Nakamura, T. Hirose, T. Ebata, Y. Yokoyama, G. Sugawara et al., Application of a three-dimensional print of a liver in hepatectomy for small tumors invisible by intraoperative ultrasonography: preliminary experience, World J. Surg. 38, 3163–3166 (2014) [CrossRef] [PubMed] [Google Scholar]
- H. Choi, G. Go, C. Lee, S.Y. Ko, S. Jeong, K. Kwon et al., Electromagnetic actuation system for locomotive intravascular therapeutic microrobot, in 5th IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics (BioRob) (IEEE, São Paulo, 2014), pp. 831–834 [CrossRef] [Google Scholar]
- D. Schmauss, S. Haeberle, C. Hagl, R. Sodian, Three-dimensional printing in cardiac surgery and interventional cardiology: a single-centre experience, Eur. J. Cardiothorac. Surg. 47, 1–9 (2014) [EDP Sciences] [PubMed] [Google Scholar]
- A. Nojiri, H. Akiyoshi, F. Ohashi, A. Ijiri, O. Sawase, T. Matsushita et al., Treatment of a unicameral bone cyst in a dog using a customized titanium device, J. Vet. Med. Sci. 77, 127 (2015) [CrossRef] [PubMed] [Google Scholar]
- R. Mayer, P. Liacouras, A. Thomas, M. Kang, L. Lin, C.B. Simone II, 3D printer generated thorax phantom with mobile tumor for radiation dosimetry, Rev. Sci. Instrum. 86, 074301 (2015) [CrossRef] [PubMed] [Google Scholar]
- M.P. Chae, D.J. Hunter-Smith, A. Rizzitelli, R.T. Spychal, W.M. Rozen, 3D volumetric analysis and haptic modeling for preoperative planning in breast reconstruction, Anaplastology 4, 138 (2015) [Google Scholar]
- K. Kondo, M. Nemoto, H. Masuda, S. Okonogi, J. Nomoto, N. Harada et al., Anatomical reproducibility of a head model molded by a three-dimensional printer, Neurol. Med. Chir. 55, 592–598 (2015) [CrossRef] [Google Scholar]
- Y. Luo, Y. Wang, B.L. Tai, R.K. Chen, A.J. Shih, Bone geometry on the contact stress in the shoulder for evaluation of pressure ulcers: finite element modeling and experimental validation, Med. Eng. Phys. 37, 187–194 (2015) [CrossRef] [PubMed] [Google Scholar]
- N. Kiarashi, A.C. Nolte, G.M. Sturgeon, W.P. Segars, S.V. Ghate, L.W. Nolte et al., Development of realistic physical breast phantoms matched to virtual breast phantoms based on human subject data, Med. Phys. 42, 4116–4126 (2015) [CrossRef] [PubMed] [Google Scholar]
- S. Isotani, Editorial comment from Dr Isotani to three-dimensional printing in urological surgery: what are the possibilities? Int. J. Urol. 22, 424 (2015) [Google Scholar]
- K. Oyama, L.F. Ditzel Filho, J. Muto, D.G. de Souza, R. Gun, B.A. Otto et al., Endoscopic endonasal cranial base surgery simulation using an artificial cranial base model created by selective laser sintering, Neurosurg. Rev. 38, 171–178 (2015) [CrossRef] [PubMed] [Google Scholar]
- M.P. Chae, D.J. Hunter-Smith, I. De-Silva, S. Tham, R.T. Spychal, W.M. Rozen, Four-dimensional (4D) printing: a new evolution in computed tomography-guided stereolithographic modeling. Principles and application, J. Reconstr. Microsurg. 31, 458–463 (2015) [Google Scholar]
- M. Rana, C.H. Chui, M. Wagner, R. Zimmerer, M. Rana, N.-C. Gellrich, Increasing the accuracy of orbital reconstruction with selective laser-melted patient-specific implants combined with intraoperative navigation, J. Oral Maxillofac. Surg. 73, 1113–1118 (2015) [CrossRef] [PubMed] [Google Scholar]
- M. Knoedler, A.H. Feibus, A. Lange, M.M. Maddox, E. Ledet, R. Thomas et al., Individualized physical 3-dimensional kidney tumor models constructed from 3-dimensional printers result in improved trainee anatomic understanding, Urology 85, 1257–1262 (2015) [Google Scholar]
- M. Kusaka, M. Sugimoto, N. Fukami, H. Sasaki, M. Takenaka, T. Anraku et al., Initial experience with a tailor-made simulation and navigation program using a 3-D printer model of kidney transplantation surgery, Transplant. Proc. 47, 596–599 (2015) [CrossRef] [PubMed] [Google Scholar]
- S.T. Bache, T. Juang, M.D. Belley, B.F. Koontz, J. Adamovics, T.T. Yoshizumi et al., Investigating the accuracy of microstereotactic-body-radiotherapy utilizing anatomically accurate 3D printed rodent-morphic dosimeters, Med. Phys. 42, 846–855 (2015) [CrossRef] [PubMed] [Google Scholar]
- A.S. Rose, J.S. Kimbell, C.E. Webster, O.L. Harrysson, E.J. Formeister, C.A. Buchman, Multi-material 3D models for temporal bone surgical simulation, Ann. Otol. Rhinol. Laryngol. 124, 528–536 (2015) [Google Scholar]
- H. Kenngott, J. Wünscher, M. Wagner, A. Preukschas, A. Wekerle, P. Neher et al., OpenHELP (Heidelberg laparoscopy phantom): development of an open-source surgical evaluation and training tool, Surg. Endosc. 29, 1–10 (2015) [Google Scholar]
- J.-C. Bernhard, S. Isotani, T. Matsugasumi, V. Duddalwar, A.J. Hung, E. Suer et al., Personalized 3D printed model of kidney and tumor anatomy: a useful tool for patient education, World J. Urol. 34, 337–345 (2015) [CrossRef] [PubMed] [Google Scholar]
- M. Azimi, E.A. Nasr, Predictive modeling of tumors using RP, in International Conference on Industrial Engineering and Operations Management (IEOM) (IEEE, Dubai, 2015), pp. 1–8 [Google Scholar]
- A.-M. Wu, Z.-X. Shao, J.-S. Wang, X.-D. Yang, W.-Q. Weng, X.-Y. Wang et al., The accuracy of a method for printing three-dimensional spinal models, PLOS ONE 10, e0124291 (2015) [CrossRef] [PubMed] [Google Scholar]
- S. Gokce, S. Gorgulu, U. Karacayli, H. Gokce, B. Battal, Three-dimensional evaluation of nasal and pharyngeal airway after Le Fort I maxillary distraction osteogenesis, Int. J. Oral Maxillofac. Surg. 44, 455–461 (2015) [CrossRef] [PubMed] [Google Scholar]
- H. Sakai, Y. Watanabe, T. Sera, H. Yokota, G. Tanaka, Visualization of particle deposition in human nasal cavities, J. Vis. 18, 349–357 (2015) [Google Scholar]
- J.R. Haaga, D. Boll, Computed Tomography & Magnetic Resonance Imaging of the Whole Body (Elsevier, Amsterdam, 2016), 6th ed. [Google Scholar]
- A. Marro, T. Bandukwala, W. Mak, Three-dimensional printing and medical imaging: a review of the methods and applications, Curr. Probl. Diagn. Radiol. 45, 2–9 (2016) [CrossRef] [PubMed] [Google Scholar]
- G. Orentlicher, A. Horowitz, D. Goldsmith, R. Delgado-Ruiz, M. Abboud, Cumulative survival rate of implants placed “fully guided” using CT-guided surgery: a 7-year retrospective study, Compend. Contin. Educ. Dent. 35, 590–600 (2014) [Google Scholar]
- H. Huang, M.-F. Hsieh, G. Zhang, H. Ouyang, C. Zeng, B. Yan et al., Improved accuracy of 3D-printed navigational template during complicated tibial plateau fracture surgery, Australas. Phys. Eng. Sci. Med. 38, 109–117 (2015) [CrossRef] [PubMed] [Google Scholar]
- R. Fürhauser, G. Mailath-Pokorny, R. Haas, D. Busenlechner, G. Watzek, B. Pommer, Esthetics of flapless single-tooth implants in the anterior maxilla using guided surgery: association of three-dimensional accuracy and pink esthetic score, Clin. Implant Dent. Relat. Res. 17, e427–e433 (2014) [CrossRef] [PubMed] [Google Scholar]
- G. Widmann, J.P.M. Berggren, B. Fischer, A.R. Pichler-Dennhardt, P. Schullian, R. Bale et al., Accuracy of image-fusion stereolithographic guides: mapping CT data with three-dimensional optical surface scannning, Clin. Implant Dent. Relat. Res. 17, e736–e744 (2015) [CrossRef] [PubMed] [Google Scholar]
- A. Reyes, I. Turkyilmaz, T.J. Prihoda, Accuracy of surgical guides made from conventional and a combination of digital scanning and rapid prototyping techniques, J. Prosthet. Dent. 113, 295–303 (2015) [CrossRef] [PubMed] [Google Scholar]
- M. Takemoto, S. Fujibayashi, E. Ota, B. Otsuki, H. Kimura, T. Sakamoto et al., Additive-manufactured patient-specific titanium templates for thoracic pedicle screw placement: novel design with reduced contact area, Eur. Spine J. 25, 1–8 (2015) [PubMed] [Google Scholar]
- D. Huang, M. Chen, D. He, C. Yang, J. Yuan, G. Bai et al., Preservation of the inferior alveolar neurovascular bundle in the osteotomy of benign lesions of the mandible using a digital template, Br. J. Oral Maxillofac. Surg. 53, 637–641 (2015) [CrossRef] [PubMed] [Google Scholar]
- Y. Li, Y. Jiang, B. Ye, J. Hu, Q. Chen, S. Zhu, Treatment of dentofacial deformities secondary to osteochondroma of the mandibular condyle using virtual surgical planning and 3-dimensional printed surgical templates, J. Oral Maxillofac. Surg. 74, 349–368 (2015) [CrossRef] [PubMed] [Google Scholar]
- S. Laycock, M. Hulse, C. Scrase, M. Tam, S. Isherwood, D. Mortimore et al., Towards the production of radiotherapy treatment shells on 3D printers using data derived from DICOM CT and MRI: preclinical feasibility studies, J. Radiother. Pract. 14, 92–98 (2015) [Google Scholar]
- R. Singh, V.K. Srivastav, B. Baby, N. Damodaran, A. Suri, A novel electro-mechanical neuro-endoscopic box trainer, in International Conference on Industrial Instrumentation and Control (ICIC) (IEEE, Pune, 2015), pp. 917–921 [CrossRef] [Google Scholar]
- D. Leordean, S. Radu, D. Frăţilă, P. Berce, Studies on design of customized orthopedic endoprostheses of titanium alloy manufactured by SLM, Int. J. Adv. Manuf. Technol. 79, 1–16 (2015) [Google Scholar]
- P. Liacouras, J. Garnes, N. Roman, A. Petrich, G.T. Grant, Designing and manufacturing an auricular prosthesis using computed tomography, 3-dimensional photographic imaging, and additive manufacturing: a clinical report, J. Prosthet. Dent. 105, 78–82 (2011) [CrossRef] [PubMed] [Google Scholar]
- R.K. Chen, Y.-A. Jin, J. Wensman, A. Shih, Additive manufacturing of custom orthoses and prostheses—a review, Addit. Manuf. 12, 77–89 (2016) [Google Scholar]
- N. Otawa, T. Sumida, H. Kitagaki, K. Sasaki, S. Fujibayashi, M. Takemoto et al., Custom-made titanium devices as membranes for bone augmentation in implant treatment: modeling accuracy of titanium products constructed with selective laser melting, J. Craniomaxillofac. Surg. 43, 1289–1295 (2015) [CrossRef] [PubMed] [Google Scholar]
- ISO 2768-1, General Tolerances—Part 1: Tolerances for Linear and Angular Dimensions Without Individual Tolerance Indications (ISO, 1989) [Google Scholar]
- V. Mironov, N. Reis, B. Derby, Review: bioprinting: a beginning, Tissue Eng. 12, 631–634 (2006) [Google Scholar]
- G.-H. Wu, S.-H. Hsu, Review: polymeric-based 3D printing for tissue engineering, J. Med. Biol. Eng. 35, 285–292 (2015) [CrossRef] [PubMed] [Google Scholar]
- X. Zhang, Y. Zhang, Tissue engineering applications of three-dimensional bioprinting, Cell Biochem. Biophys. 72, 772–782 (2015) [Google Scholar]
- N. Xu, X. Ye, D. Wei, J. Zhong, Y. Chen, G. Xu et al., 3D artificial bones for bone repair prepared by computed tomography-guided fused deposition modeling for bone repair, ACS Appl. Mater. Interfaces 6, 14952–14963 (2014) [Google Scholar]
- A.L. Jardini, M.A. Larosa, R. Maciel Filho, C.A. de Carvalho Zavaglia, L.F. Bernardes, C.S. Lambert et al., Cranial reconstruction: 3D biomodel and custom-built implant created using additive manufacturing, J. Craniomaxillofac. Surg. 42, 1877–1884 (2014) [CrossRef] [PubMed] [Google Scholar]
- H. Radovan, J. Ziak, T. Teodor, M. Jaroslav, L.K. Martin, Evaluation of custom-made implants using industrial computed tomography, in 10th International Conference on Digital Technologies (DT) (IEEE, Zilina, 2014), pp. 82–86 [Google Scholar]
- M. Cronskär, On Customization of Orthopedic Implants—From Design and Additive Manufacturing to Implementation, PhD Thesis, Mid Sweden University, Östersund, Sweden, 2014 [Google Scholar]
- X. Li, H. Cai, X. Cui, P. Cao, J. Zhang, G. Li et al., Prevention of late postpneumonectomy complications using a 3D printed lung in dog models, Eur. J. Cardiothorac. Surg. 46, e67–e73 (2014) [CrossRef] [PubMed] [Google Scholar]
- G. Rasperini, S. Pilipchuk, C. Flanagan, C. Park, G. Pagni, S. Hollister et al., 3D-printed bioresorbable scaffold for periodontal repair, J. Dent. Res. 94, 153S–157S (2015) [CrossRef] [PubMed] [Google Scholar]
- S.F.S. Shirazi, S. Gharehkhani, M. Mehrali, H. Yarmand, H.S.C. Metselaar, N.A. Kadri et al., A review on powder-based additive manufacturing for tissue engineering: selective laser sintering and inkjet 3D printing, Sci. Technol. Adv. Mater. 16, 033502 (2015) [Google Scholar]
- E. Farré-Guasch, J. Wolff, M.N. Helder, E.A.J.M. Schulten, T. Forouzanfar, J. Klein-Nulend, Application of additive manufacturing in oral and maxillofacial surgery, J. Oral Maxillofac. Surg. 73, 2408–2418 (2015) [CrossRef] [PubMed] [Google Scholar]
- S. van Uden, J. Silva-Correia, V. Correlo, J. Oliveira, R. Reis, Custom-tailored tissue engineered polycaprolactone scaffolds for total disc replacement, Biofabrication 7, 015008 (2015) [CrossRef] [PubMed] [Google Scholar]
- A. Maru, Evaluating the Use of 3D Imaging in Creating a Canal-Directed Endodontic Access, Master's Thesis, Indiana University, Indianapolis, IN, USA, 2015 [Google Scholar]
- Y. Li, W. Yang, X. Li, X. Zhang, C. Wang, X. Meng et al., Improving osteointegration and osteogenesis of three-dimensional porous Ti6Al4V scaffolds by polydopamine-assisted biomimetic hydroxyapatite coating, ACS Appl. Mater. Interfaces 7, 5715–5724 (2015) [Google Scholar]
- W. Mroz, B. Budner, R. Syroka, K. Niedzielski, G. Golański, A. Slósarczyk et al., In vivo implantation of porous titanium alloy implants coated with magnesium-doped octacalcium phosphate and hydroxyapatite thin films using pulsed laser depostion, J. Biomed. Mater. Res. B: Appl. Biomater. 103, 151–158 (2015) [CrossRef] [Google Scholar]
- H.R. Cho, T.S. Roh, K.W. Shim, Y.O. Kim, D.H. Lew, I.S. Yun, Skull reconstruction with custom made three-dimensional titanium implant, Arch. Craniofac. Surg. 16, 11–16 (2015) [Google Scholar]
- M. Haefeli, D. Schaefer, R. Schumacher, M. Müller-Gerbl, P. Honigmann, Titanium template for scaphoid reconstruction, J. Hand Surg. Eur. 40, 526–533 (2014) [CrossRef] [Google Scholar]
- E. Vorndran, C. Moseke, U. Gbureck, 3D printing of ceramic implants, MRS Bull. 40, 127–136 (2015) [Google Scholar]
- C. Lueders, B. Jastram, R. Hetzer, H. Schwandt, Rapid manufacturing techniques for the tissue engineering of human heart valves, Eur. J. Cardiothorac. Surg. 46, 593–601 (2014) [CrossRef] [PubMed] [Google Scholar]
- X. Wang, S. Xu, S. Zhou, W. Xu, M. Leary, P. Choong et al., Topological design and additive manufacturing of porous metals for bone scaffolds and orthopaedic implants: a review, Biomaterials 83, 127–141 (2016) [CrossRef] [PubMed] [Google Scholar]
Cite this article as: Adam Thompson, Donal McNally, Ian Maskery, Richard K. Leach, X-ray computed tomography and additive manufacturing in medicine: a review, Int. J. Metrol. Qual. Eng. 8, 17 (2017)
All Tables
All Figures
 |
Fig. 1 The SLS, FDM and SLA processes, respectively [3]. |
| In the text | |
 |
Fig. 2 Schematic diagrams of the five generations of medical XCT scanner [9]. |
| In the text | |
|
Fig. 3 The first combined use of XCT and AM, producing an SLA skull model. Mankovitch et al. noted in the model the depiction of a cleft upper palate and the presence of imaging artefacts around the teeth in the XCT data, induced by the presence of incomplete attenuation profiles as a result of the patient's metal fillings [9]. Build problems were also noted in the B image relating to floating contours and the nature of the SLA process. Images reproduced from reference [12]. |
| In the text | |
|
Fig. 4 Bottom, side and top views of surface rendered XCT data, showing bone formation around a render of the STL used to produce the implanted scaffold, as well as an individual XCT slice showing cortical shell and trabeculae within marrow spaces. Images reproduced from reference [36]. |
| In the text | |
|
Fig. 5 Left to right: pre-operative, immediately post-operative and six months post-operative XCT scans of first human AM implant. Images reproduced from reference [54]. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.